Physiotherapy For Severs Disease
Overview
Sever disease refers to a calcaneal apophysitis (an inflammation of the apophysis of the heel) which occurs in children and young adolescents. It typically presents in active young children (especially ones who engage in jumping and running sports).
Causes
At birth, most of our foot bones are still made of cartilage, which ossifies (becomes bony) over the first few years of life. At the back of the heel, there is a growth plate that is attached to the main body of the heel bone by a cartilaginous join. At about the age of 14-15 years, this area of cartilage between the growth plate and the heel bone ossifies, fusing the area to the heel. Sever?s disease occurs when there is too much motion or strain across the growth plate, resulting in this area becoming inflamed and painful.
Symptoms
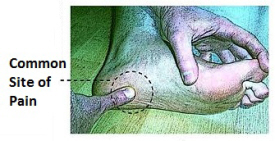
The most common symptoms of Sever?s involves pain or tenderness in one or both heels. This pain usually occurs at the back of the heel, but can also extend to the sides and bottom of the heel. A child with Sever?s may also have these common problems, Heel pain with limping, especially after running. Difficulty walking, Discomfort or stiffness in the feet upon awaking. Swelling and redness in the heel, Symptoms are usually worse during or after activity and get better with rest.
Diagnosis
It is not difficult for a doctor to diagnose Sever's disease in a youngster or teenager. A personal history and a physical examination are usually all it takes to determine the cause of heel pain.
Non Surgical Treatment
stretching exercises can help. It is important that your child performs exercises to stretch the hamstring and calf muscles, and the tendons on the back of the leg. The child should do these stretches 2 or 3 times a day. Each stretch should be held for about 20 seconds. Both legs should be stretched, even if the pain is only in 1 heel. Your child also needs to do exercises to strengthen the muscles on the front of the shin. To do this, your child should sit on the floor, keeping his or her hurt leg straight. One end of a bungee cord or piece of rubber tubing is hooked around a table leg. The other end is hitched around the child's toes. The child then scoots back just far enough to stretch the cord. Next, the child slowly bends the foot toward his or her body. When the child cannot bend the foot any closer, he or she slowly points the foot in the opposite direction (toward the table). This exercise (15 repetitions of "foot curling") should be done about 3 times. The child should do this exercise routine a few times daily.
Sever disease refers to a calcaneal apophysitis (an inflammation of the apophysis of the heel) which occurs in children and young adolescents. It typically presents in active young children (especially ones who engage in jumping and running sports).
Causes
At birth, most of our foot bones are still made of cartilage, which ossifies (becomes bony) over the first few years of life. At the back of the heel, there is a growth plate that is attached to the main body of the heel bone by a cartilaginous join. At about the age of 14-15 years, this area of cartilage between the growth plate and the heel bone ossifies, fusing the area to the heel. Sever?s disease occurs when there is too much motion or strain across the growth plate, resulting in this area becoming inflamed and painful.
Symptoms
The most common symptoms of Sever?s involves pain or tenderness in one or both heels. This pain usually occurs at the back of the heel, but can also extend to the sides and bottom of the heel. A child with Sever?s may also have these common problems, Heel pain with limping, especially after running. Difficulty walking, Discomfort or stiffness in the feet upon awaking. Swelling and redness in the heel, Symptoms are usually worse during or after activity and get better with rest.
Diagnosis
It is not difficult for a doctor to diagnose Sever's disease in a youngster or teenager. A personal history and a physical examination are usually all it takes to determine the cause of heel pain.
Non Surgical Treatment
stretching exercises can help. It is important that your child performs exercises to stretch the hamstring and calf muscles, and the tendons on the back of the leg. The child should do these stretches 2 or 3 times a day. Each stretch should be held for about 20 seconds. Both legs should be stretched, even if the pain is only in 1 heel. Your child also needs to do exercises to strengthen the muscles on the front of the shin. To do this, your child should sit on the floor, keeping his or her hurt leg straight. One end of a bungee cord or piece of rubber tubing is hooked around a table leg. The other end is hitched around the child's toes. The child then scoots back just far enough to stretch the cord. Next, the child slowly bends the foot toward his or her body. When the child cannot bend the foot any closer, he or she slowly points the foot in the opposite direction (toward the table). This exercise (15 repetitions of "foot curling") should be done about 3 times. The child should do this exercise routine a few times daily.
Acquired Flat Foot Tibialis Posterior Dysfunction
Overview
The posterior tibial tendon serves as one of the major supporting structures of the foot, helping it to function while walking. Posterior tibial tendon dysfunction (PTTD) is a condition caused by changes in the tendon, impairing its ability to support the arch. This results in flattening of the foot. PTTD is often called ?adult acquired flatfoot? because it is the most common type of flatfoot developed during adulthood. Although this condition typically occurs in only one foot, some people may develop it in both feet. PTTD is usually progressive, which means it will keep getting worse, especially if it isn?t treated early. 
Causes
There are numerous causes of acquired adult flatfoot, including fracture or dislocation, tendon laceration, tarsal coalition, arthritis, neuroarthropathy, neurologic weakness, and iatrogenic causes. The most common cause of acquired adult flatfoot is posterior tibial tendon dysfunction.
Symptoms
Posterior tibial tendon insufficiency is divided into stages by most foot and ankle specialists. In stage I, there is pain along the posterior tibial tendon without deformity or collapse of the arch. The patient has the somewhat flat or normal-appearing foot they have always had. In stage II, deformity from the condition has started to occur, resulting in some collapse of the arch, which may or may not be noticeable. The patient may feel it as a weakness in the arch. Many patients initially present in stage II, as the ligament failure can occur at the same time as the tendon failure and therefore deformity can already be occurring as the tendon is becoming symptomatic. In stage III, the deformity has progressed to the extent where the foot becomes fixed (rigid) in its deformed position. Finally, in stage IV, deformity occurs at the ankle in addition to the deformity in the foot.
Diagnosis
First, both feet should be examined with the patient standing and the entire lower extremity visible. The foot should be inspected from above as well as from behind the patient, as valgus angulation of the hindfoot is best appreciated when the foot is viewed from behind. Johnson described the so-called more-toes sign: with more advanced deformity and abduction of the forefoot, more of the lateral toes become visible when the foot is viewed from behind. The single-limb heel-rise test is an excellent determinant of the function of the posterior tibial tendon. The patient is asked to attempt to rise onto the ball of one foot while the other foot is suspended off the floor. Under normal circumstances, the posterior tibial muscle, which inverts and stabilizes the hindfoot, is activated as the patient begins to rise onto the forefoot. The gastrocnemius-soleus muscle group then elevates the calcaneus, and the heel-rise is accomplished. With dysfunction of the posterior tibial tendon, however, inversion of the heel is weak, and either the heel remains in valgus or the patient is unable to rise onto the forefoot. If the patient can do a single-limb heel-rise, the limb may be stressed further by asking the patient to perform this maneuver repetitively.
Non surgical Treatment
Patients can be treated non-surgically with in-shoe devices and braces to hold their feet in the correct position. This can reduce pain and damage and assist with walking. Physical therapy is also given to improve muscle strength and help prevent injury to the foot. Surgery can be performed if the patient doesn?t find any relief. 
Surgical Treatment
If cast immobilization fails, surgery is the next alternative. Treatment goals include eliminating pain, halting deformity progression and improving mobility. Subtalar Arthroereisis, 15 minute outpatient procedure, may correct flexible flatfoot deformity (hyperpronation). The procedure involves placing an implant under the ankle joint (sinus tarsi) to prevent abnormal motion. Very little recovery time is required and it is completely reversible if necessary. Ask your Dallas foot doctor for more information about this exciting treatment possibility.
What Causes Heel Soreness
Overview

More than 20 percent of patients visit foot specialists because of Heel Pain, and approximately one-third of all patients I see come because of this problem. Over 50 percent of Americans will experience heel pain during their lifetime. The most common form of heel pain is known as plantar fasciitis or "heel spur syndrome." The plantar fascia is a thick ligament on the bottom of your foot spanning from your heel to the base of your toes. It supports the arch and several muscles under the bones that support the foot. Overtime, most people will develop some degree of calcification within these muscles on the bottom of their heel called a "spur."
Causes
In our pursuit of healthy bodies, pain can be an enemy. In some instances, however, it is of biological benefit. Pain that occurs right after an injury or early in an illness may play a protective role, often warning us about the damage we've suffered. When we sprain an ankle, for example, the pain warns us that the ligament and soft tissues may be frayed and bruised, and that further activity may cause additional injury. Pain, such as may occur in our heels, also alerts us to seek medical attention. This alert is of utmost importance because of the many afflictions that contribute to heel pain.
Symptoms
Pain typically comes on gradually, with no injury to the affected area. It is frequently triggered by wearing a flat shoe, such as flip-flop sandals. Flat footwear may stretch the plantar fascia to such an extent that the area becomes swollen (inflamed). In most cases, the pain is under the foot, toward the front of the heel. Post-static dyskinesia (pain after rest) symptoms tend to be worse just after getting out of bed in the morning, and after a period of rest during the day. After a bit of activity symptoms often improve a bit. However, they may worsen again toward the end of the day.
Diagnosis
After you have described your foot symptoms, your doctor will want to know more details about your pain, your medical history and lifestyle, including. Whether your pain is worse at specific times of the day or after specific activities. Any recent injury to the area. Your medical and orthopedic history, especially any history of diabetes, arthritis or injury to your foot or leg. Your age and occupation. Your recreational activities, including sports and exercise programs. The type of shoes you usually wear, how well they fit, and how frequently you buy a new pair. Your doctor will examine you, including. An evaluation of your gait. While you are barefoot, your doctor will ask you to stand still and to walk in order to evaluate how your foot moves as you walk. An examination of your feet. Your doctor may compare your feet for any differences between them. Then your doctor may examine your painful foot for signs of tenderness, swelling, discoloration, muscle weakness and decreased range of motion. A neurological examination. The nerves and muscles may be evaluated by checking strength, sensation and reflexes. In addition to examining you, your health care professional may want to examine your shoes. Signs of excessive wear in certain parts of a shoe can provide valuable clues to problems in the way you walk and poor bone alignment. Depending on the results of your physical examination, you may need foot X-rays or other diagnostic tests.
Non Surgical Treatment
Treatment for plantar fasciitis - the vast majority of patients recover with conservative treatments (designed to avoid radical medical therapeutic measures or operative procedures) within months. Heel with ice-pack. Home care such as rest, ice-pack use, proper-fitting footwear and foot supports are often enough to ease heel pain. Non-steroidal anti-inflammatory drugs (NSAIDs) - medications with analgesic (pain reducing), antipyretic (fever reducing) effects. In higher doses they also have anti-inflammatory effects, they reduce inflammation (swelling). Non-steroidal distinguishes NSAIDs from other drugs which contain steroids, which are also anti-inflammatory. NSAIDs are non-narcotic (they do not induce stupor). For patients with plantar fasciitis they may help with pain and inflammation. Corticosteroids, a corticosteroid solution is applied over the affected area on the skin; an electric current is used to help absorption. Alternatively, the doctor may decide to inject the medication. However, multiple injections may result in a weakened plantar fascia, significantly increasing the risk of rupture and shrinkage of the fat pad covering the heel bone. Some doctors may use ultrasound to help them make sure they have injected in the right place Corticosteroids are usually recommended when NSAIDs have not helped. Physical therapy, a qualified/specialized physical therapist (UK: physiotherapist) can teach the patient exercises which stretch the plantar fascia and Achilles tendon, as well as strengthening the lower leg muscles, resulting in better stabilization of the ankle and heel. The patient may also be taught how to apply athletic taping, which gives the bottom of the foot better support. Night splints, the splint is fitted to the calf and foot; the patient keeps it on during sleep. Overnight the plantar fascia and Achilles tendon are held in a lengthened position; this stretches them. Orthotics, insoles and orthotics (assistive devices) can be useful to correct foot faults, as well as cushioning and cradling the arch during the healing process. Extracorporeal shock wave therapy, sound waves are aimed at the affected area to encourage and stimulate healing. This type of therapy is only recommended for chronic (long-term) cases, which have not responded to conservative therapy.
Surgical Treatment
When a diagnosis of plantar fasciitis is made early, most patients respond to conservative treatment and don?t require surgical intervention. Often, when there is a secondary diagnosis contributing to your pain, such as an entrapped nerve, and you are non-responsive to conservative care, surgery may be considered. Dr. Talarico will discuss all options and which approach would be the most beneficial for your condition.
Prevention
It may not be possible to prevent all cases of heel pain. However, there are some easy steps that you can take to avoid injury to the heel and prevent pain. Whenever possible, you should wear shoes that fit properly and support the foot, wear the right shoes for physical activity, stretch your muscles before exercising, pace yourself during physical activity, maintain a healthy diet, rest when you feel tired or when your muscles ache, maintain a healthy weight.
More than 20 percent of patients visit foot specialists because of Heel Pain, and approximately one-third of all patients I see come because of this problem. Over 50 percent of Americans will experience heel pain during their lifetime. The most common form of heel pain is known as plantar fasciitis or "heel spur syndrome." The plantar fascia is a thick ligament on the bottom of your foot spanning from your heel to the base of your toes. It supports the arch and several muscles under the bones that support the foot. Overtime, most people will develop some degree of calcification within these muscles on the bottom of their heel called a "spur."
Causes
In our pursuit of healthy bodies, pain can be an enemy. In some instances, however, it is of biological benefit. Pain that occurs right after an injury or early in an illness may play a protective role, often warning us about the damage we've suffered. When we sprain an ankle, for example, the pain warns us that the ligament and soft tissues may be frayed and bruised, and that further activity may cause additional injury. Pain, such as may occur in our heels, also alerts us to seek medical attention. This alert is of utmost importance because of the many afflictions that contribute to heel pain.
Symptoms
Pain typically comes on gradually, with no injury to the affected area. It is frequently triggered by wearing a flat shoe, such as flip-flop sandals. Flat footwear may stretch the plantar fascia to such an extent that the area becomes swollen (inflamed). In most cases, the pain is under the foot, toward the front of the heel. Post-static dyskinesia (pain after rest) symptoms tend to be worse just after getting out of bed in the morning, and after a period of rest during the day. After a bit of activity symptoms often improve a bit. However, they may worsen again toward the end of the day.
Diagnosis
After you have described your foot symptoms, your doctor will want to know more details about your pain, your medical history and lifestyle, including. Whether your pain is worse at specific times of the day or after specific activities. Any recent injury to the area. Your medical and orthopedic history, especially any history of diabetes, arthritis or injury to your foot or leg. Your age and occupation. Your recreational activities, including sports and exercise programs. The type of shoes you usually wear, how well they fit, and how frequently you buy a new pair. Your doctor will examine you, including. An evaluation of your gait. While you are barefoot, your doctor will ask you to stand still and to walk in order to evaluate how your foot moves as you walk. An examination of your feet. Your doctor may compare your feet for any differences between them. Then your doctor may examine your painful foot for signs of tenderness, swelling, discoloration, muscle weakness and decreased range of motion. A neurological examination. The nerves and muscles may be evaluated by checking strength, sensation and reflexes. In addition to examining you, your health care professional may want to examine your shoes. Signs of excessive wear in certain parts of a shoe can provide valuable clues to problems in the way you walk and poor bone alignment. Depending on the results of your physical examination, you may need foot X-rays or other diagnostic tests.
Non Surgical Treatment
Treatment for plantar fasciitis - the vast majority of patients recover with conservative treatments (designed to avoid radical medical therapeutic measures or operative procedures) within months. Heel with ice-pack. Home care such as rest, ice-pack use, proper-fitting footwear and foot supports are often enough to ease heel pain. Non-steroidal anti-inflammatory drugs (NSAIDs) - medications with analgesic (pain reducing), antipyretic (fever reducing) effects. In higher doses they also have anti-inflammatory effects, they reduce inflammation (swelling). Non-steroidal distinguishes NSAIDs from other drugs which contain steroids, which are also anti-inflammatory. NSAIDs are non-narcotic (they do not induce stupor). For patients with plantar fasciitis they may help with pain and inflammation. Corticosteroids, a corticosteroid solution is applied over the affected area on the skin; an electric current is used to help absorption. Alternatively, the doctor may decide to inject the medication. However, multiple injections may result in a weakened plantar fascia, significantly increasing the risk of rupture and shrinkage of the fat pad covering the heel bone. Some doctors may use ultrasound to help them make sure they have injected in the right place Corticosteroids are usually recommended when NSAIDs have not helped. Physical therapy, a qualified/specialized physical therapist (UK: physiotherapist) can teach the patient exercises which stretch the plantar fascia and Achilles tendon, as well as strengthening the lower leg muscles, resulting in better stabilization of the ankle and heel. The patient may also be taught how to apply athletic taping, which gives the bottom of the foot better support. Night splints, the splint is fitted to the calf and foot; the patient keeps it on during sleep. Overnight the plantar fascia and Achilles tendon are held in a lengthened position; this stretches them. Orthotics, insoles and orthotics (assistive devices) can be useful to correct foot faults, as well as cushioning and cradling the arch during the healing process. Extracorporeal shock wave therapy, sound waves are aimed at the affected area to encourage and stimulate healing. This type of therapy is only recommended for chronic (long-term) cases, which have not responded to conservative therapy.
Surgical Treatment
When a diagnosis of plantar fasciitis is made early, most patients respond to conservative treatment and don?t require surgical intervention. Often, when there is a secondary diagnosis contributing to your pain, such as an entrapped nerve, and you are non-responsive to conservative care, surgery may be considered. Dr. Talarico will discuss all options and which approach would be the most beneficial for your condition.
Prevention
It may not be possible to prevent all cases of heel pain. However, there are some easy steps that you can take to avoid injury to the heel and prevent pain. Whenever possible, you should wear shoes that fit properly and support the foot, wear the right shoes for physical activity, stretch your muscles before exercising, pace yourself during physical activity, maintain a healthy diet, rest when you feel tired or when your muscles ache, maintain a healthy weight.
What's The Major Cause Of Achilles Tendonitis ?
Overview
 Achilles tendonitis is an iInflammation in the tendon of the calf muscle, where it attaches to the heel bone. Achilles tendonitis causes pain and stiffness at the back of the leg, near the heel. Achilles tendonitis can be caused by overuse of the Achilles tendon, overly tight calf muscles or Achilles tendons, excess uphill running, a sudden increase in the intensity of training or the type of shoes worn to run, or wearing high heels at work and then switching to a lower-heeled workout shoe. Achilles tendonitis causes pain, tenderness, and often swelling over the Achilles tendon. There is pain on rising up on the toes and pain with stretching of the tendon. The range of motion of the ankle may be limited. Treatment includes applying ice packs to the Achilles tendon, raising the lower leg, and taking an anti-inflammatory medication. In some severe cases of Achilles tendonitis, a cast may be needed for several weeks. A heel lift insert may also be used in shoes to prevent future overstretching of the Achilles tendon. Exerting rapid stress on the Achilles tendon when it is inflamed can result in rupture of the tendon.
Achilles tendonitis is an iInflammation in the tendon of the calf muscle, where it attaches to the heel bone. Achilles tendonitis causes pain and stiffness at the back of the leg, near the heel. Achilles tendonitis can be caused by overuse of the Achilles tendon, overly tight calf muscles or Achilles tendons, excess uphill running, a sudden increase in the intensity of training or the type of shoes worn to run, or wearing high heels at work and then switching to a lower-heeled workout shoe. Achilles tendonitis causes pain, tenderness, and often swelling over the Achilles tendon. There is pain on rising up on the toes and pain with stretching of the tendon. The range of motion of the ankle may be limited. Treatment includes applying ice packs to the Achilles tendon, raising the lower leg, and taking an anti-inflammatory medication. In some severe cases of Achilles tendonitis, a cast may be needed for several weeks. A heel lift insert may also be used in shoes to prevent future overstretching of the Achilles tendon. Exerting rapid stress on the Achilles tendon when it is inflamed can result in rupture of the tendon.
Causes
Hill running or stair climbing. Overuse resulting from the natural lack of flexibility in the calf muscles. Rapidly increasing mileage or speed. Starting up too quickly after a layoff. Trauma caused by sudden and hard contraction of the calf muscles when putting out extra effort such as in a final sprint. Achilles tendinitis often begins with mild pain after exercise or running that gradually worsens.
Symptoms
Common symptoms of Achilles tendinitis include, pain and stiffness along the Achilles tendon in the morning, pain along the tendon or back of the heel that worsens with activity, Severe pain the day after exercising, thickening of the tendon, bone spur (insertional tendinitis) swelling that is present all the time and gets worse throughout the day with activity, If you have experienced a sudden "pop" in the back of your calf or heel, you may have ruptured (torn) your Achilles tendon. See your doctor immediately if you think you may have torn your tendon.
Diagnosis
The diagnosis is made via discussion with your doctor and physical examination. Typically, imaging studies are not needed to make the diagnosis. However, in some cases, an ultrasound is useful in looking for evidence of degenerative changes in the tendon and to rule out tendon rupture. An MRI can be used for similar purposes, as well. Your physician will determine whether or not further studies are necessary.
Nonsurgical Treatment
To help heal your Achille?s Tendinitis, follow the R.I.C.E. Principle including Rest, Ice Compression and Elevation. In addition your physiotherapist will likely recommend specific exercises promote healing and strengthening of the Achilles tendon and its supporting structures. As well an orthotic that elevates your heel can reduce stress on your Achilles tendon. Reducing inflammation in the tendon is important too this can often be achieved with oral pills or topical creams. Over-the-counter pain medications or prescription strength such as ibuprofen. However, these drugs can have side effects, like an increased risk of bleeding ulcers. They should be used only occasionally unless your doctor specifically says otherwise. Topical anti-inflammatory creams made with natural ingredients designed specifically for feet and legs (eg ZAX?s Original Heelspur Cream ) target the affected areas and provides effective and safe relief. Tendinitis usually responds well to self-care measures. But if your signs and symptoms are severe or persistent, your doctor might suggest other treatment options including surgery.

Surgical Treatment
Histological and biological studies on tendon healing have made it possible to envisage surgical repair using a percutaneous approach, with the following objectives, a minimal, and not very aggressive, operation, which is quick and easy and within the capabilities of all surgeons, the shortest hospitalisation period possible, above all, early and effective re-education, providing a satisfactory result both in terms of solidity and the comfort of the patient. The percutaneous tenosynthesis TENOLIG combines stability, reliability, patient comfort and lower overall social and professional costs for this type of lesion.
Prevention
If you're just getting started with your training, be sure to stretch after running, and start slowly, increasing your mileage by no more than 10% per week. Strengthen your calf muscles with exercises such as toe raises. Work low-impact cross-training activities, such as cycling and swimming, into your training.
Achilles tendonitis is an iInflammation in the tendon of the calf muscle, where it attaches to the heel bone. Achilles tendonitis causes pain and stiffness at the back of the leg, near the heel. Achilles tendonitis can be caused by overuse of the Achilles tendon, overly tight calf muscles or Achilles tendons, excess uphill running, a sudden increase in the intensity of training or the type of shoes worn to run, or wearing high heels at work and then switching to a lower-heeled workout shoe. Achilles tendonitis causes pain, tenderness, and often swelling over the Achilles tendon. There is pain on rising up on the toes and pain with stretching of the tendon. The range of motion of the ankle may be limited. Treatment includes applying ice packs to the Achilles tendon, raising the lower leg, and taking an anti-inflammatory medication. In some severe cases of Achilles tendonitis, a cast may be needed for several weeks. A heel lift insert may also be used in shoes to prevent future overstretching of the Achilles tendon. Exerting rapid stress on the Achilles tendon when it is inflamed can result in rupture of the tendon.
Causes
Hill running or stair climbing. Overuse resulting from the natural lack of flexibility in the calf muscles. Rapidly increasing mileage or speed. Starting up too quickly after a layoff. Trauma caused by sudden and hard contraction of the calf muscles when putting out extra effort such as in a final sprint. Achilles tendinitis often begins with mild pain after exercise or running that gradually worsens.
Symptoms
Common symptoms of Achilles tendinitis include, pain and stiffness along the Achilles tendon in the morning, pain along the tendon or back of the heel that worsens with activity, Severe pain the day after exercising, thickening of the tendon, bone spur (insertional tendinitis) swelling that is present all the time and gets worse throughout the day with activity, If you have experienced a sudden "pop" in the back of your calf or heel, you may have ruptured (torn) your Achilles tendon. See your doctor immediately if you think you may have torn your tendon.
Diagnosis
The diagnosis is made via discussion with your doctor and physical examination. Typically, imaging studies are not needed to make the diagnosis. However, in some cases, an ultrasound is useful in looking for evidence of degenerative changes in the tendon and to rule out tendon rupture. An MRI can be used for similar purposes, as well. Your physician will determine whether or not further studies are necessary.
Nonsurgical Treatment
To help heal your Achille?s Tendinitis, follow the R.I.C.E. Principle including Rest, Ice Compression and Elevation. In addition your physiotherapist will likely recommend specific exercises promote healing and strengthening of the Achilles tendon and its supporting structures. As well an orthotic that elevates your heel can reduce stress on your Achilles tendon. Reducing inflammation in the tendon is important too this can often be achieved with oral pills or topical creams. Over-the-counter pain medications or prescription strength such as ibuprofen. However, these drugs can have side effects, like an increased risk of bleeding ulcers. They should be used only occasionally unless your doctor specifically says otherwise. Topical anti-inflammatory creams made with natural ingredients designed specifically for feet and legs (eg ZAX?s Original Heelspur Cream ) target the affected areas and provides effective and safe relief. Tendinitis usually responds well to self-care measures. But if your signs and symptoms are severe or persistent, your doctor might suggest other treatment options including surgery.
Surgical Treatment
Histological and biological studies on tendon healing have made it possible to envisage surgical repair using a percutaneous approach, with the following objectives, a minimal, and not very aggressive, operation, which is quick and easy and within the capabilities of all surgeons, the shortest hospitalisation period possible, above all, early and effective re-education, providing a satisfactory result both in terms of solidity and the comfort of the patient. The percutaneous tenosynthesis TENOLIG combines stability, reliability, patient comfort and lower overall social and professional costs for this type of lesion.
Prevention
If you're just getting started with your training, be sure to stretch after running, and start slowly, increasing your mileage by no more than 10% per week. Strengthen your calf muscles with exercises such as toe raises. Work low-impact cross-training activities, such as cycling and swimming, into your training.
What Is Painful Heel

Overview
Plantar fasciitis is a very common condition resulting in pain under the heel which often radiates into the foot. We explain free of charge everything you need to know to cure your pain and prevent it from returning.
Causes
You are more likely to develop plantar fasciitis if you are Active, sports that place excessive stress on the heel bone and attached tissue, especially if you have tight calf muscles or a stiff ankle from a previous ankle sprain, which limits ankle movement eg. Running, ballet dancing and aerobics. Overweight. Carrying around extra weight increases the strain and stress on your plantar fascia. Pregnant. The weight gain and swelling associated with pregnancy can cause ligaments to become more relaxed, which can lead to mechanical problems and inflammation. On your feet. Having a job that requires a lot of walking or standing on hard surfaces ie factory workers, teachers and waitresses. Flat Feet or High Foot Arches. Changes in the arch of your foot changes the shock absorption ability and can stretch and strain the plantar fascia, which then has to absorb the additional force. Middle-Aged or Older. With ageing the arch of your foot may begin to sag - putting extra stress on the plantar fascia. Wearing shoes with poor support. Weak Foot Arch Muscles. Muscle fatigue allows your plantar fascia to overstress and cause injury. Arthritis. Some types of arthritis can cause inflammation in the tendons in the bottom of your foot, which may lead to plantar fasciitis. Diabetes. Although doctors don't know why, plantar fasciitis occurs more often in people with diabetes.
Symptoms
Plantar fasciitis sufferers feel a sharp stab or deep ache in the middle of the heel or along the arch. Another sign is the morning hobble from the foot trying to heal itself in a contracted position overnight. Taking that first step causes sudden strain on the bottom of the foot. The pain can recur after long spells of sitting, but it tends to fade during a run, once the area is warmed up.
Diagnosis
To diagnose plantar fasciitis, your doctor will physically examine your foot by testing your reflexes, balance, coordination, muscle strength, and muscle tone. Your doctor may also advise a magnetic resonance imaging (MRI) or X-ray to rule out other others sources of your pain, such as a pinched nerve, stress fracture, or bone spur.
Non Surgical Treatment
Reducing inflammation in the plantar fascia ligament is an important part of treatment, though this does not address the underlying damage to the ligament. Initial home treatment includes staying off your feet and applying ice for 15 to 20 minutes three or four times a day to reduce swelling. You can also try reducing or changing your exercise activities. Using arch supports in your shoes and doing stretching exercises may also help to relieve pain. Nonsteroidal anti-inflammatory drugs (NSAIDS), such as ibuprofen (i.e. Motrin or Advil) and naproxen (i.e. Aleve), are often used to reduce inflammation in the ligament. If home treatments and over-the-counter anti-inflammatory drugs don’t ease the pain, an injection of a corticosteroid directly into the damaged section of the ligament can be given. Your doctor can do this in his or her office. Your doctor may use an ultrasound device to help determine the best place for the injection. Corticosteroids can also be administered on the skin of your heel or the arch of your foot, and then a painless electrical current is applied to let the steroid pass through your skin and into the muscle. Physical therapy is an important part of treatment for planter fasciitis. It can help stretch your plantar fascia and Achilles tendons. A physical therapist can also show you exercises to strengthen your lower leg muscles, helping to stabilize your walk and lessen the workload on your plantar fascia. If pain continues and other methods aren’t working, your doctor may recommend extracorporeal shock wave therapy. Sound waves are bombarded against your heel to stimulate healing within the ligament. This treatment can result in bruises, swelling, pain, and numbness, and has not been proven to be consistently effective in relieving symptoms.
Surgical Treatment
Surgery should be reserved for patients who have made every effort to fully participate in conservative treatments, but continue to have pain from plantar fasciitis. Patients should fit the following criteria. Symptoms for at least 9 months of treatment. Participation in daily treatments (exercises, stretches, etc.). If you fit these criteria, then surgery may be an option in the treatment of your plantar fasciitis. Unfortunately, surgery for treatment of plantar fasciitis is not as predictable as a surgeon might like. For example, surgeons can reliably predict that patients with severe knee arthritis will do well after knee replacement surgery about 95% of the time. Those are very good results. Unfortunately, the same is not true of patients with plantar fasciitis.
Stretching Exercises
Calf stretch. Lean forward against a wall with one knee straight and the heel on the ground. Place the other leg in front, with the knee bent. To stretch the calf muscles and the heel cord, push your hips toward the wall in a controlled fashion. Hold the position for 10 seconds and relax. Repeat this exercise 20 times for each foot. A strong pull in the calf should be felt during the stretch. Plantar fascia stretch. This stretch is performed in the seated position. Cross your affected foot over the knee of your other leg. Grasp the toes of your painful foot and slowly pull them toward you in a controlled fashion. If it is difficult to reach your foot, wrap a towel around your big toe to help pull your toes toward you. Place your other hand along the plantar fascia. The fascia should feel like a tight band along the bottom of your foot when stretched. Hold the stretch for 10 seconds. Repeat it 20 times for each foot. This exercise is best done in the morning before standing or walking.
What Exactly Causes Heel Discomfort

Overview
To find out where this condition gets its name, we need to look at a specific area of the foot. Your foot is made up of bones, muscles, tendons, and ligaments. The plantar fascia is a relatively inflexible, strong, fibrous band on the bottom of the foot that supports the arch of your foot. Beginning at the heel bone, the plantar fascia extends the length of your foot to connect with your toes at the ball of the foot. When you walk, your weight is distributed across your feet. Any imbalances in the mechanics of your foot and distribution of weight can potentially cause pain. Diseases involving inflammation end with "itis." This explains the name of the condition as being an inflammation of the plantar fascia, thus plantar fasciitis. Repetitive movements such as walking or running stretch the plantar fascia. Because it is not very flexible, this can cause small tears in the fascia, which leads to inflammation and pain. Other factors such as high arches, fallen arches, or a change in the walking surface contribute to the stress placed on the plantar fascia and heel.
Causes
Under normal circumstances, your plantar fascia acts like a shock-absorbing bowstring, supporting the arch in your foot. If tension on that bowstring becomes too great, it can create small tears in the fascia. Repetitive stretching and tearing can cause the fascia to become irritated or inflamed.
Symptoms
Among the symptoms for Plantar Fasciitis is pain usually felt on the underside of the heel, often most intense with the first steps after getting out of bed in the morning. It is commonly associated with long periods of weight bearing or sudden changes in weight bearing or activity. Plantar Fasciitis also called “policeman’s heel” is presented by a sharp stabbing pain at the bottom or front of the heel bone. In most cases, heel pain is more severe following periods of inactivity when getting up and then subsides, turning into a dull ache.
Diagnosis
During the physical exam, your doctor checks for points of tenderness in your foot. The location of your pain can help determine its cause. Usually no tests are necessary. The diagnosis is made based on the history and physical examination. Occasionally your doctor may suggest an X-ray or magnetic resonance imaging (MRI) to make sure your pain isn't being caused by another problem, such as a stress fracture or a pinched nerve. Sometimes an X-ray shows a spur of bone projecting forward from the heel bone. In the past, these bone spurs were often blamed for heel pain and removed surgically. But many people who have bone spurs on their heels have no heel pain.
Non Surgical Treatment
Most doctors recommend an initial six- to eight-week program of conservative treatment, including Rest, balanced with stretching exercises to lengthen the heel cord and plantar fascia. Ice massage to the bottom of the foot after activities that trigger heel pain. Avoidance of walking barefoot or wearing slippers or sandals that provide little arch support. A temporary switch to swimming and/or bicycling instead of sports that involve running and jumping. Shoes with soft heels and insoles. Taping the bottom of the injured foot. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen (Advil, Motrin and other brand names), or acetaminophen (Tylenol) for pain. Physical therapy using ultrasound, electrical stimulation with corticosteroids or massage techniques. If this conservative treatment does not help, your doctor may recommend that you wear a night splint for six to eight weeks. While you sleep, the night splint will keep your foot in a neutral or slightly flexed (bent) position to help maintain the normal stretch of the plantar fascia and heel cord. If the night splint doesn't work, your doctor may inject corticosteroid medication into the painful area or place your foot in a short leg cast for one to three months. Shock wave therapy, in which focused sound energy is applied to the sore heel, may be recommended for plantar fasciitis. The shock waves are intended to irritate or injure the plantar fascia to promote healing. The overall benefit of this approach is uncertain. Other therapies that have been tried include radiation therapy and botulinum toxin injections. But their effectiveness is unclear. If all else fails, your doctor may suggest surgery. But this is rare, and surgery is not always successful.

Surgical Treatment
Surgery for plantar fasciitis can be very successful in the right patients. While there are potential complications, about 70-80% of patients will find relief after plantar fascia release surgery. This may not be perfect, but if plantar fasciitis has been slowing you down for a year or more, it may well be worth these potential risks of surgery. New surgical techniques allow surgery to release the plantar fascia to be performed through small incisions using a tiny camera to locate and cut the plantar fascia. This procedure is called an endoscopic plantar fascia release. Some surgeons are concerned that the endoscopic plantar fascia release procedure increases the risk of damage to the small nerves of the foot. While there is no definitive answer that this endoscopic plantar fascia release is better or worse than a traditional plantar fascia release, most surgeons still prefer the traditional approach.
What Causes Pain In The Heel And The Way To Deal With It

Overview
The plantar fascia is a band of connective tissue that runs along the sole from the heel to the ball of the foot. One of its main roles is to keep the bones and joints in position. Bruising or overstretching this ligament can cause inflammation and heel pain. A common cause is flat feet, because the ligament is forced to overstretch as the foot spreads out and the arch flattens. The pain may be worse first thing in the morning or after rest. In many cases, plantar fasciitis is associated with heel spur. The plantar fascia tears and bleeds at the heel and, over time, these injuries calcify and form a bony growth.
Causes
Plantar fasciitis can be confused with a condition called tarsal tunnel syndrome. In tarsal tunnel syndrome, an important nerve in the foot, the tibial nerve, is trapped and pinched as it passes through the tarsal tunnel, a condition analogous to carpal tunnel syndrome in the wrist. This may cause symptoms similar to the pain of a plantar fasciitis. There are also other less common problems such as nerve entrapments, stress fractures, and fat pad necrosis, all of which can cause foot pain. Finally, several rheumatologic conditions can cause heel pain. These syndromes such as Reiter's syndrome and ankylosing spondylitis can cause heel pain similar to plantar fasciitis. If your symptoms are not typical for plantar fasciitis, or if your symptoms do not resolve with treatment, your doctor will consider these possible diagnoses.
Symptoms
Plantar fasciitis generally occurs in one foot. Bilateral plantar fasciitis is unusual and tends to be the result of a systemic arthritic condition that is exceptionally rare among athletes. Males suffer from a somewhat greater incidence of plantar fasciitis than females, perhaps as a result of greater weight coupled with greater speed and ground impact, as well as less flexibility in the foot. Typically, the sufferer of plantar fasciitis experiences pain upon rising after sleep, particularly the first step out of bed. Such pain is tightly localized at the bony landmark on the anterior medial tubercle of the calcaneus. In some cases, pain may prevent the athlete from walking in a normal heel-toe gait, causing an irregular walk as means of compensation. Less common areas of pain include the forefoot, Achilles tendon, or subtalar joint. After a brief period of walking, the pain usually subsides, but returns again either with vigorous activity or prolonged standing or walking. On the field, an altered gait or abnormal stride pattern, along with pain during running or jumping activities are tell-tale signs of plantar fasciitis and should be given prompt attention. Further indications of the injury include poor dorsiflexion (lifting the forefoot off the ground) due to a shortened gastroc complex, (muscles of the calf). Crouching in a full squat position with the sole of the foot flat on the ground can be used as a test, as pain will preclude it for the athlete suffering from plantar fasciitis, causing an elevation of the heel due to tension in the gastroc complex.
Diagnosis
Plantar fasciitis is usually diagnosed by a health care provider after consideration of a person’s presenting history, risk factors, and clinical examination. Tenderness to palpation along the inner aspect of the heel bone on the sole of the foot may be elicited during the physical examination. The foot may have limited dorsiflexion due to tightness of the calf muscles or the Achilles tendon. Dorsiflexion of the foot may elicit the pain due to stretching of the plantar fascia with this motion. Diagnostic imaging studies are not usually needed to diagnose plantar fasciitis. However, in certain cases a physician may decide imaging studies (such as X-rays, diagnostic ultrasound or MRI) are warranted to rule out other serious causes of foot pain. Bilateral heel pain or heel pain in the context of a systemic illness may indicate a need for a more in-depth diagnostic investigation. Lateral view x-rays of the ankle are the recommended first-line imaging modality to assess for other causes of heel pain such as stress fractures or bone spur development. Plantar fascia aponeurosis thickening at the heel greater than 5 millimeters as demonstrated by ultrasound is consistent with a diagnosis of plantar fasciitis. An incidental finding associated with this condition is a heel spur, a small bony calcification on the calcaneus (heel bone), which can be found in up to 50% of those with plantar fasciitis. In such cases, it is the underlying plantar fasciitis that produces the heel pain, and not the spur itself. The condition is responsible for the creation of the spur though the clinical significance of heel spurs in plantar fasciitis remains unclear.
Non Surgical Treatment
Your GP or podiatrist may advise you to change your footwear. You should avoid wearing flat-soled shoes, because they will not provide your heel with support and could make your heel pain worse. Ideally, you should wear shoes that cushion your heels and provide a good level of support to the arches of your feet. For women wearing high heels, and for men wearing heeled boots or brogues, can provide short- to medium-term pain relief, as they help reduce pressure on the heels. However, these types of shoes may not be suitable in the long term, because they can lead to further episodes of heel pain. Your GP or podiatrist can advise on footwear. Orthoses are insoles that fit inside your shoe to support your foot and help your heel recover. You can buy orthoses off-the-shelf from sports shops and larger pharmacies. Alternatively, your podiatrist should be able to recommend a supplier. If your pain does not respond to treatment and keeps recurring, or if you have an abnormal foot shape or structure, custom-made orthoses are available. These are specifically made to fit the shape of your feet. However, there is currently no evidence to suggest that custom-made orthoses are more effective than those bought off-the-shelf. An alternative to using orthoses is to have your heel strapped with sports strapping (zinc oxide) tape, which helps relieve pressure on your heel. Your GP or podiatrist can teach you how to apply the tape yourself. In some cases, night splints can also be useful. Most people sleep with their toes pointing down, which means tissue inside the heel is squeezed together. Night splints, which look like boots, are designed to keep your toes and feet pointing up while you are asleep. This will stretch both your Achilles tendon and your plantar fascia, which should help speed up your recovery time. Night splints are usually only available from specialist shops and online retailers. Again, your podiatrist should be able to recommend a supplier. If treatment hasn't helped relieve your painful symptoms, your GP may recommend corticosteroid injections. Corticosteroids are a type of medication that have a powerful anti-inflammatory effect. They have to be used sparingly because overuse can cause serious side effects, such as weight gain and high blood pressure (hypertension). As a result, it is usually recommended that no more than three corticosteroid injections are given within a year in any part of the body. Before having a corticosteroid injection, a local anaesthetic may be used to numb your foot so you don't feel any pain.

Surgical Treatment
Surgery is not a common treatment for this condition. Approximately 5% of people with plantar fasciitis require surgery if non-surgical methods do not help to relieve pain within a year. The surgical procedure involves making an incision in the plantar fascia in order to decrease the tension of the ligament. Potential risks of this surgical procedure include irritation of the nerves around the heel, continued plantar fasciitis, heel or foot pain, infection, flattening of the arch, problems relating to the anesthetic.
Prevention
Plantar fasciitis can be a nagging problem, which gets worse and more difficult to treat the longer it's present. To prevent plantar fasciitis, run on soft surfaces, keep mileage increases to less than 10 percent per week, and visit a specialty running shop to make sure you're wearing the proper shoes for your foot type and gait. It's also important to stretch the plantar fascia and Achilles tendon.